Identifying Left Bundle Branch Block
It is never more important in emergency medicine than when it comes into contact with cardiology. In the field this will be the role of the Paramedic and in the Emergency Room it is the role of the Nursing Staff and the Emergency room Physician. I purposely put the Nursing Staff before the Emergency Physician, because they are the ones with the ER techs that do the Emergent 12 Lead EKG on the patient. It is also my belief coming from a Paramedic background into Emergency Nursing that Emergency Nurses should be very adept at reading 12 Lead EKG's. It is ultimately the Emergency Physician's responsibility to diagnose, but we are part of the team and should be able to help the Physician when they may have many critical patients they are caring for.
In caring for the cardiac patient, the nemesis is the chest pain rule out MI, in the presence of Left Bundle Branch Block. So let us take a look at the process of identifying Left Bundle Branch Block (LBBB).
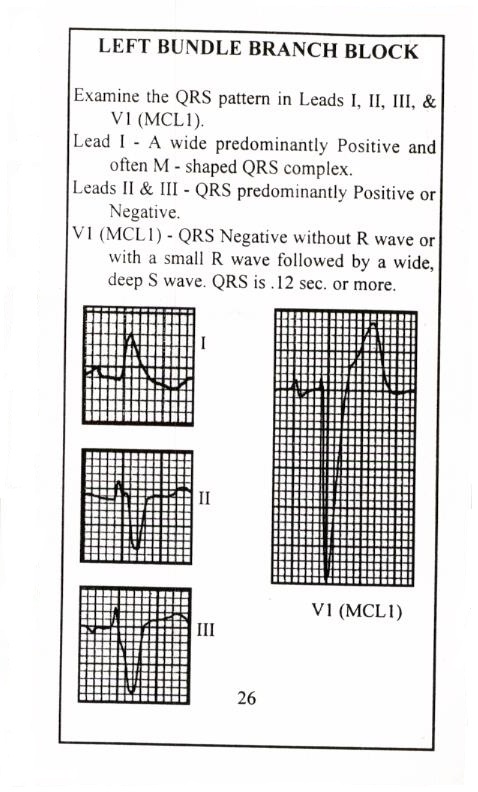
In the setting of a cardiac patient having chest pain, as you know the first question when faced with the patient having a left bundle is whether or not it is new or old. If it is a new LBBB, it is pathological and can be a sign of a myocardial infarction. It is difficult to diagnose myocardial infarction in the presence of LBBB, due to the fact that the baseline ST segments and T waves tend to be shifted in a discordant direction, which can mask or mimic acute myocardial infarction. We now have the modified Sgarbossa Criteria to help us in the diagnosis of an acute myocardial infarction in the presence of LBBB.
Modified Sgarbossa
