LinkExchange Member
Reasons Why Not To Use Lead II
In 1991 a study was done in San Francisco evaluating the diagnostic yield from leads V1, V6, MCL1 and MCL6 compared to Lead 2. Using Lead 2 the diagnosis was correctly made in only 34% of wide QRS tachycardias. However a correct diagnosis was achieved in 75 to 80% with each of the precordial leads.
A. Globally unlike either BBB (Marriott)
B. V Leads: None with RS complex/ Any RS > 0.10s (Brugada :1991)
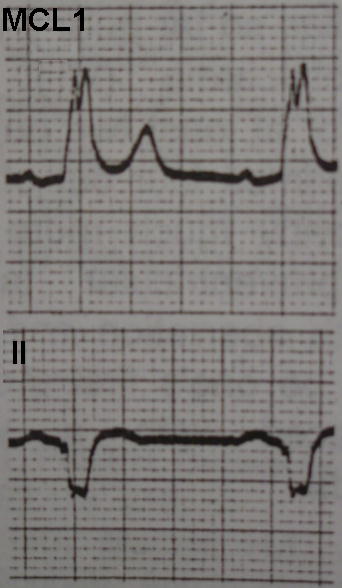
C. Single Lead: V1 - qR or R with Lt Rabbitt Ear (Gozensky/Thorne : 1974)
Single Peak (known as steeple)(Wellens/Brugada : 1987)
QR or Equiphasic RS
Fat R, slurred downstroke to late nadir(tip) >.06s(1.5 baby blocks)
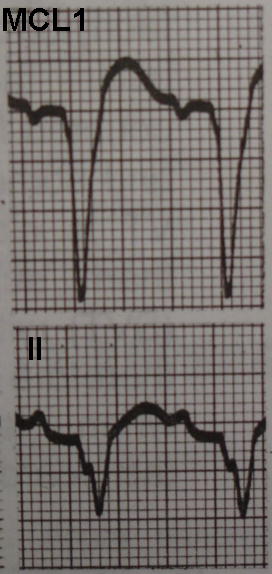
V6 - rS, equiphasic QS or QR complex
S or QS > 15mm deep
A. Axis in no mans land : Neg Complex I, AVF, or I, II, III
Concordance positive or negative of chest leads V1 - V6 ( exceptions *** wpw can produce Pos concordance/ LBBB with LAD may produce Neg concordance)
2. Polarity
Now you can see why it is so important to monitor a critical patient in a lead that will give you more information. If you have the capability to monitor more than just one lead that is all the better, however if you can only monitor one lead at a time, MCL1 is the preferred lead due to the amount of information you can obtain.
