LinkExchange Member
An Introduction to MCL1
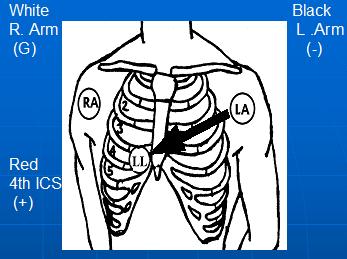
If you are using a three lead EKG machine, apply 4 electrodes to the patient: Rt arm (white), Lt arm (black), Lt leg (red), & 4th IC space. Then run a 6 second strip of leads I,II,III, & then move the left leg wire (red) to the chest lead, leaving your monitor on lead III. This will give you MCL1.
If you are using a three lead EKG machine, and your monitor switch is set on the typical lead II monitoring lead: simply reverse your arm leads: white on left, black on right, and then place your red on the 4th intercostal space right sternal border.
If you are using a five lead EKG machine, apply 5 electrodes to the patient: Rt arm (white), Lt arm (black), Rt leg (green), Lt leg (red), 4th IC space (brown),(assuming typical colors for a five lead cable). You then have to go to your selector switch and select the lead you wish to monitor.
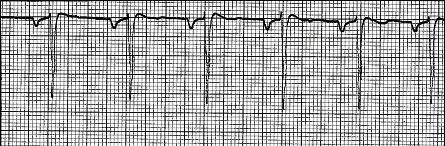
When monitoring patients, we should monitor them in a lead that gives us the most information about disturbances of rhythm and conduction and that would be V1 or MCL1 and not lead II.
The advantages of monitoring in MCL1 compared to Lead II include:
1. You can immediately distinguish between left ventricular ectopy (where QRS is mostly positive, and also has a greater propensity to give you R on T phenomenon..ie Ventricular Fibrillation) and right ventricular ectopy (where QRS is mostly negative) in most cases.
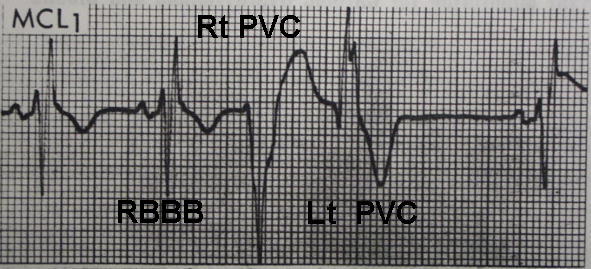
**Notice the "rabbitt ears" in Lt PVC, this only applies to MCL1 lead!!!!
2. You can tell right bundle branch from left bundle branch.
3. P waves are more easily seen in right sided monitoring leads.
4. Most importantly monitoring in MCL1 gives you the information you need for the differential diagnosis between ventricular tachycardia and aberration.
The disadvantages of MCL1 is that it fails to recognize shifts of axis and the polarity of the p wave is not as informative as it is in lead II, (sinus p wave in MCL1 when it is diphasic is usually +-, and the ectopic or retrograde p wave is -+)