If we examine the limb leads we see that there is ST elevation in his inferior leads: II,III,AVF. Indicating that this is an Acute Inferior MI.
If we look at lead I, there is no noticeable ST segment changes, and lead AVL shows slight inversion of T wave.
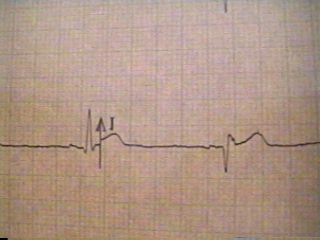
Now we turn our attention to the chest leads and look at those. In lead V1, we have a positive complex and an inverted T wave, hmmm...
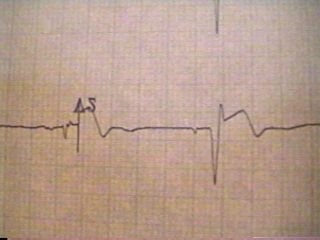
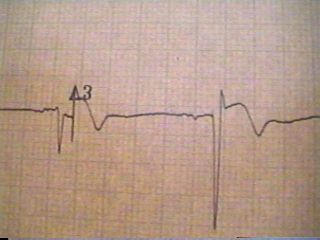
In V2-V3 we have very noticeable ST segment depressions.
The question now is, are these representative of "reciprocal changes" from the inferior injury pattern or is it an "injury pattern" itself.
The answer lies in V1...you have a positive "R" wave, with ST depression. A prominent "R" wave in V1 may represent any of the following:
Posterior MI
Rt. Vt. Hypertrophy
Rt. Bundle Branch Block
Wolf Parkinson White Syndrome
If we take the EKG in hand and turn it over and hold it up to a light source, we now see, the "mirror image" of the EKG, showing us elevated ST segments in V1-V3. So this EKG, would be read as an acute inferior/posterior MI. See images below for "mirror image".